Humanized Mouse Models: Core Technical Considerations
Translating therapeutic breakthroughs from the lab bench to the clinic is one of the steepest hurdles in modern drug discovery. Traditional murine models, while invaluable, often fall short when evaluating human-specific immunotherapies, biologicals, and viral pathogens. The human immune system simply speaks a different molecular language.
Enter humanized mouse models-animals engineered to harbor human cells, tissues, or functional immune systems. While these models bridge the translational gap, establishing them is less of a standard laboratory protocol and more of a highly sensitive biological art. Microscopic variations in host genetics, graft processing, or pre-conditioning can mean the difference between robust human cell engraftment and a costly experimental failure.
Here is a deep technical dive into the critical parameters required to establish highly reproducible humanized mouse models.
Selecting the Optimal Immunodeficient Host
The success of any human xenotransplantation relies entirely on the host's inability to reject foreign tissue. The field has evolved far beyond the classic nude or SCID mice, which still retained residual innate immunity.
The Genetic Architecture of Deep Deficiency
Modern humanized studies rely on severely immunocompromised backgrounds, most notably the NSG (NOD.C57BL/6-italic*Prkdcscid IL2rgtm1Wjl*/SzJ) or NCG strains. These models combine the Prkdc mutation (which eliminats mature T and B cells) with a targeted knockout of the interleukin-2 receptor gamma chain (IL2rg). The loss of the γ-chain completely halts the signaling of multiple interleukins, effectively preventing the development of Natural Killer (NK) cells. Without NK cells, the host's primary innate defense against xenogeneic grafts is dismantled.
Next-Generation Transgenic Variants
Standard NSG mice support human lymphocyte engraftment but fail to sustain specific lineages due to a lack of cross-species cytokine support. When choosing a host, match the strain to your therapeutic target:
- Myeloid Development: Strains like NSG-SGM3 trans-genically express human SCF, GM-CSF, and IL-3, promoting the differentiation of human myeloid cells, monocytes, and dendritic cells.
- Antigen Presentation: If your therapy relies on MHC-restricted T-cell activation, models expressing human HLA alleles (e.g., NSG-HLA-A2/DR4) ensure that engrafted human T cells are properly educated and functional.
Graft Sources and Pre-conditioning Standardizations
The blueprint of your humanized immune system depends entirely on the graft source. The two most common approaches-Peripheral Blood Mononuclear Cells (PBMCs) and CD34+ Hematopoietic Stem Cells (HSCs)-offer distinct biological windows.
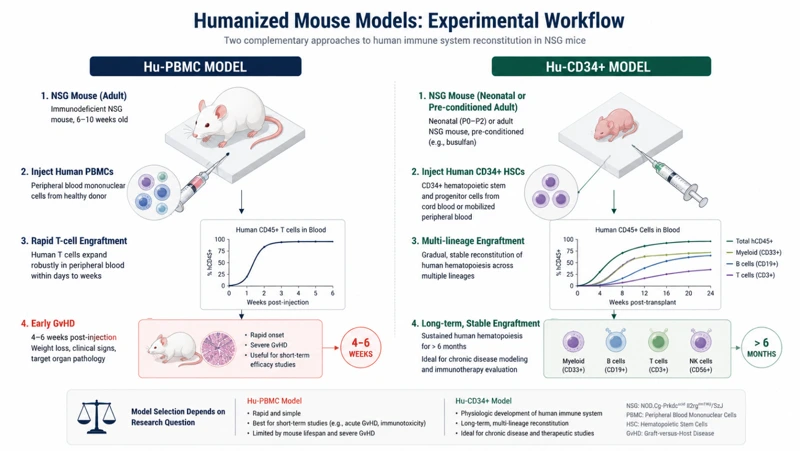
Hu-PBMC vs. Hu-CD34+ Models
- Hu-PBMC Models: Created by injecting mature human PBMCs into adult mice. This provides a rapid, cost-effective model rich in mature human T cells, ideal for short-term oncology studies. However, because these mature human cells recognize the mouse tissue as foreign, Xenogeneic Graft-versus-Host Disease (GvHD) typically sets in within 4 to 6 weeks, limiting the experimental window.
- Hu-CD34+ Models: Created by injecting multi-potent HSCs (isolated from umbilical cord blood or mobilized bone marrow) into neonatal or pre-conditioned adult mice. This leads to a multi-lineage, long-term human immune system with low GvHD risk, though it requires months to mature.
The Logistics of Pre-conditioning
To allow human HSCs to home to the murine bone marrow niche, the host's existing hematopoietic cells must be cleared. This is achieved via sub-lethal irradiation or chemotherapy (such as Busulfan).
- Precision is mandatory: If the radiation dose is too low, host cells recover and outcompete the human graft. If it is too high, the mouse develops severe gastrointestinal toxicity.
- Quality Control: Always verify the viability of thawed CD34+ cells prior to injection. A cell viability score below 90% or a magnetic bead selection purity below 95% will drastically compromise engraftment kinetics.
Technical Execution and Surgical Rigor
Once the host is prepared and the graft is verified, the physical delivery of cells demands flawless technique.
Injection Routes and Volumes
For neonatal mice (typically used in CD34+ protocols within 24-48 hours of birth), intrahepatic (IH) or intracardiac (IC) injections are preferred to maximize stem cell homing. In adult mice, tail vein intravenous (IV) or retro-orbital (RO) delivery is standard.
- Care must be taken to limit injection volumes (typically maxing out at 200 uL for adult IV) and to avoid cell aggregation. Clogged cell suspensions can cause micro-embolisms in the mouse pulmonary vasculature, leading to immediate post-injection mortality.
Maintaining the Microbiological Shield
Severely immunocompromised mice are extraordinarily fragile. Opportunistic pathogens like Pseudomonas aeruginosa or Pneumocystis jirovecii, which wouldn't cause a sneeze in a wild-type mouse, are lethal here.
- Operate under strict sterile hood conditions during handling and injections.
- Provide prophylactic antibiotic regimens (e.g., sulfamethoxazole/trimethoprim or acidified water) during the critical weeks surrounding pre-conditioning and engraftment.
Monitoring and Quantifying Reconstruction
An animal is not truly "humanized" until flow cytometry confirms functional, circulating human leukocytes.
Standardizing the Flow Gating Strategy
Routinely sample peripheral blood starting at weeks 8 to 12 post-engraftment. A robust multicolor flow cytometry panel must include a clear distinction between human CD45 (hCD45) and mouseCD45 (mCD45). The ratio of hCD45+ / (hCD45+ + mCD45+) determines the overall chimerism percentage.
Total Leukocytes --> Separate hCD45+ vs. mCD45+ --> Gating Lineages (CD3+, CD19+, CD14+)
Once the hCD45+ baseline is established, evaluate multi-lineage differentiation using specific markers:
- T cells: CD3+ (sub-gated into CD4+ helper and CD8+ cytotoxic populations)
- B cells: CD19+ or CD20+
- Monocytes/Myeloid cells: CD14+ or CD11b+
Defining the Success Threshold
Establish a clear, mathematical cutoff for your experimental cohorts. For long-term tumor efficacy or infectious disease studies using CD34+ models, a chimerism threshold of hCD45+ ≥ 25% in peripheral blood at week 12 is generally considered a fully humanized, study-ready animal. Any mice falling below this threshold should be excluded before group assignment to minimize baseline data noise.
Conclusion
Building a reliable humanized mouse model is a balancing act of genetic selection, cellular quality control, and pristine surgical execution. By systematically standardizing your host choices, optimizing pre-conditioning windows, and utilizing strict flow cytometry gating thresholds, you transform a highly variable biological system into a robust, high-fidelity platform for translational science.
Creative Bioarray Relevant Recommendations
| Products & Services | Description |
|---|---|
| Humanized Mouse Models | Creative Bioarray enhances your preclinical immuno-oncology research endeavors by offering state-of-the-art humanized mouse model solutions that are tailored to target specific human immune responses. |
| Humanized PBMC Mouse Models | Creative Bioarray has successfully established highly stable humanized PBMC mouse models, tailored for our clients to evaluate the efficacy of immune therapies in tumor treatment. |
| Humanized CD34+ HSC Models | Creative Bioarray has successfully engineered sophisticated humanized mouse model featuring CD34+ hematopoietic stem cells (HSCs), meticulously designed for cutting-edge drug efficacy studies. |