Comparing Plasma Protein Binding Methods
Total plasma concentration of a drug (free plus protein bound) is not always a reliable indicator in drug discovery. The most important parameter is the unbound fraction (fu), representing the fraction of drug not bound to plasma proteins such as albumin or alpha-1-acid glycoprotein. This free fraction alone can traverse cell membranes, bind therapeutic targets, and undergo clearance.
Accurate determination of plasma protein binding (PPB) is a key element of early DMPK assessment. However, using an inappropriate assay can generate artifactual data that may confound downstream estimates of in vivo efficacy and PK/PD modelling. In this post we compare the major drug binding assays head-to-head to help match the appropriate approach to the specific chemistry of your pipeline.
Head-to-Head Comparison of the Big Three PPB Approaches
In the bioanalytical field, three main approaches are used to distinguish free drug from protein-bound complexes. Each is based on a different separation principle, with distinct trade-offs in terms of throughput, speed, and susceptibility to analytical artifacts.
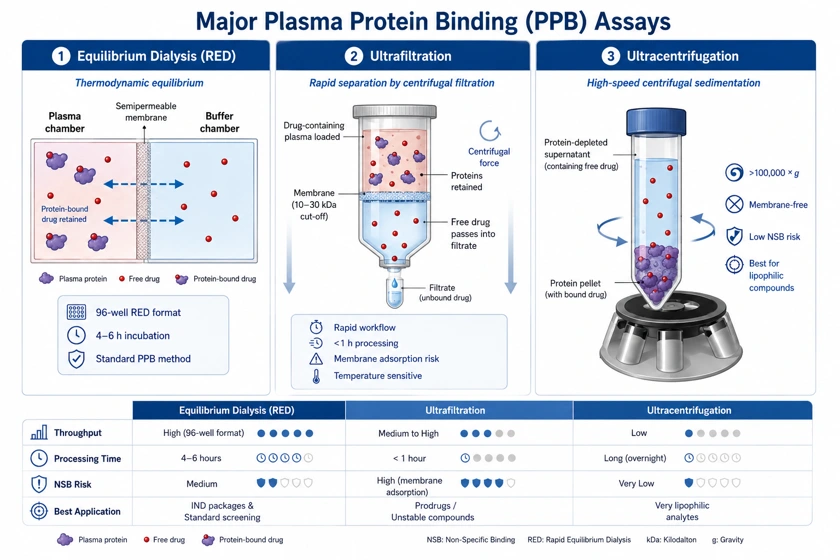
| Evaluation Metric | Equilibrium Dialysis (RED) | Ultrafiltration | Ultracentrifugation |
|---|---|---|---|
| Primary Driver | Thermodynamic Equilibrium | Centrifugal Filtration | High-Speed Centrifugal Sedimentation |
| Throughput | High (96-well format) | Medium to High | Low |
| Processing Time | 4 to 6 hours | < 1 hour | Long (overnight) |
| Non-Specific Binding Risk | Medium | High (Membrane adsorption) | Very Low |
| Best Used For | IND packages & Standard screening | Prodrugs/Unstable compounds | Very lipophilic analytes |
Equilibrium Dialysis (Gold Standard)
Equilibrium dialysis is the gold standard recognized by major regulatory agencies. In this experiment, a semipermeable membrane separates a plasma chamber from a buffer chamber. The free drug crosses the membrane until thermodynamic equilibrium is reached between the two compartments.
- The Evolution: Dialysis using traditional dialysis cells was historically labor-intensive. Modern High-Throughput Equilibrium Dialysis, especially Rapid Equilibrium Dialysis (RED) systems, has simplified the process into standardized 96-well automation-friendly plates with incubation durations of approximately 4-6 hours.
Ultrafiltration
Ultrafiltration is not an equilibrium process. Instead, drug-containing plasma is placed in a filter unit with a defined molecular weight cut-off (usually 10-30 kDa) and centrifuged. Centrifugal force drives the unbound drug in the aqueous ultrafiltrate through the membrane while retaining the larger plasma proteins.
- The Trade-off: Although very rapid, ultrafiltration is highly sensitive to temperature variations and membrane fouling, both of which can affect filtration rates and distort results.
Ultracentrifugation (The Membrane-Free Alternative)
This approach is completely membrane-free. Plasma samples are spun at very high speeds (sometimes exceeding 100,000 × g for several hours), physically forcing proteins to the bottom of the tube as a pellet. The clear, protein-depleted supernatant is then carefully removed and analyzed for free drug concentration.
Critical Evaluation: Equilibrium Dialysis vs Ultrafiltration
Researchers typically need to balance analytical speed and equilibrium accuracy when choosing between the two most widely used high-throughput approaches.
- The Stability Challenge: If a development candidate is chemically or enzymatically unstable in plasma (e.g., certain prodrugs), it may degrade during a 4 to 6 hours equilibrium dialysis run at 37℃. In such cases, the rapid workflow of ultrafiltration becomes important, even though method validation requirements may be more stringent.
- Volume Changes and Dilution Effects: Equilibrium dialysis is vulnerable to water shifts in which water transfers from the buffer chamber into the hyperosmotic plasma chamber during incubation. This dilutes plasma proteins and can result in overestimation of the observed fu. Validated assays should account for this shift using post-dialysis mass balance calculations. On the other hand, collecting excessive ultrafiltrate volume can create concentration effects that may influence the binding equilibrium during centrifugation. Best practices typically limit ultrafiltration to collecting less than 10% of the total sample volume.
Dealing with Common PPB Problems
Reproducible PPB data requires deliberate mitigation of three frequent experimental artifacts:
Handling Drugs with High Binding (fu < 1%)
For contemporary, highly lipophilic small molecules, the unbound fraction can be extremely low (e.g., fu = 0.002). At this level, the buffer chamber concentration may fall below the lower limit of quantification (LLOQ) of conventional LC-MS/MS assays. To address this, laboratories may employ matrix-dilution approaches (e.g., diluting plasma 10-fold to artificially increase the free fraction, followed by back-calculation using the law of mass action) in conjunction with ultra-sensitive targeted mass spectrometry techniques.
Counteracting Non-Specific Binding (NSB)
Lipophilic compounds tend to adsorb to plastic housing and semipermeable membranes. For compounds with significant NSB in equilibrium dialysis, drug loss from both plasma and buffer phases may result in incomplete mass balance recovery (< 80%). To prevent this, membranes may be pre-treated with anti-adsorptive agents or low-binding polymers may be used. To identify NSB artifacts, mass balance (Volumeplasma × Concplasma + Volumebuffer × Concbuffer) should be monitored for every compound.
Tight pH Control
Upon exposure to air, text CO2 escapes from plasma and plasma pH may gradually increase. This change in pH affects both the ionization state of the drug and the conformation of plasma proteins, potentially altering the observed binding affinity. All equilibrium dialysis incubations should be conducted within a specialized 5% CO2 incubator, or the plasma should be buffered with a physiological modifier (e.g., 100 mM sodium phosphate) to maintain pH at 7.4.
Pipeline Decision Matrix
- Early Screening (Discovery): Utilize high-throughput RED devices. The objective is to rank compound libraries and eliminate assets with excessively high or low binding liabilities.
- Lead Optimisation & IND-Enabling Studies: Perform extensive multi-species equilibrium dialysis (rat, mouse, dog, non-human primate, human) with complete mass balance accounting and precise pH control to generate data suitable for regulatory submissions.
- Special Modalities: For unstable esters or rapidly degrading prodrugs, switch early to ultrafiltration at 4℃ to capture the binding profile before degradation occurs.
Conclusion
Plasma protein binding is not a checkbox assay. Selection among equilibrium dialysis, ultrafiltration, and ultracentrifugation should be dictated by the physicochemical and metabolic properties of the compound itself. By choosing the appropriate assay design for a molecule's specific chemistry, experimental artifacts can be minimized and reliable free-drug data can be generated to support progression into clinical development.
Creative Bioarray Relevant Recommendations
| Products & Services | Description |
|---|---|
| Plasma Protein Binding Assay | Our Plasma Protein Binding (PPB) Assay provides accurate measurement of unbound drug fractions across species, supporting PK/PD evaluation and safety margin assessment. |