How to Select the Right Humanized Mouse Model for Immuno-Oncology
The transition from in vitro discovery to in vivo validation is one of the most critical inflection points in drug development. In immuno-oncology (IO), this step has historically been plagued by a frustrating bottleneck: the mouse immune system is fundamentally different from that of a human. From distinct T-cell receptor signaling pathways to contrasting cytokine profiles, traditional murine models often fail to predict how a novel biologic will behave in patients. The consequence? Promising candidates hit a brick wall during Phase I clinical trials.
Humanized mouse models-immunodeficient mice reconstituted with human immune cells or engineered to express human drug targets-have bridged this translational chasm. However, there is no single "perfect" humanized model. Choosing the wrong host system can lead to premature graft-versus-host disease (GvHD), poorly synchronized immune cell maturation, or misallocated research budgets.
To help you optimize your preclinical strategy, this guide deconstructs the major humanized platforms, maps them to specific therapeutic modalities, and exposes the critical nuances that separate a successful study from a compromised one.
The Three Pillars of Humanized Mouse Models
To select the ideal model, you must first understand the biological architecture, operational timelines, and inherent trade-offs of the three primary platforms available today.
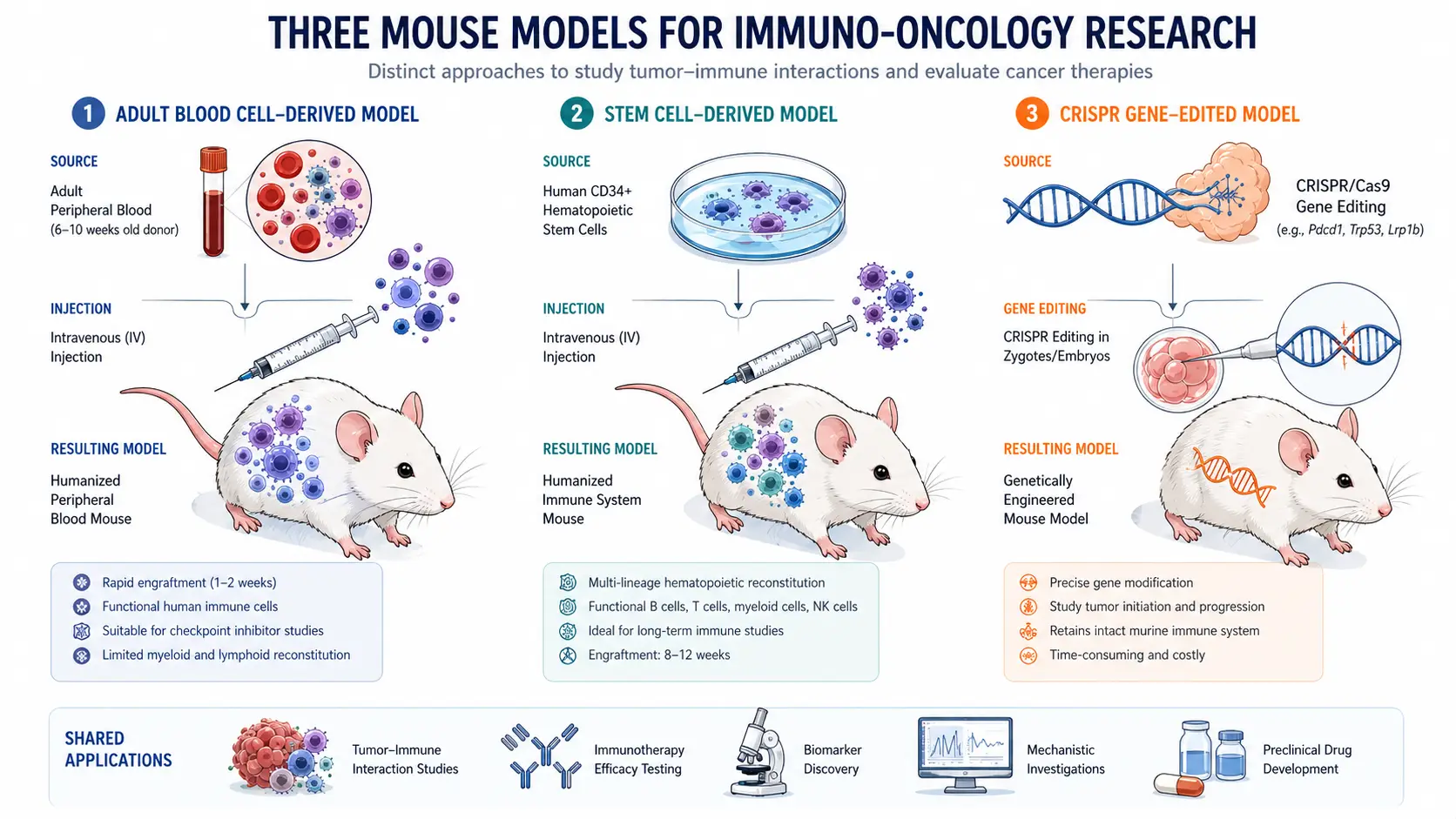
The hu-PBMC Model
The hu-PBMC model is generated by injecting adult human peripheral blood mononuclear cells into severely immunodeficient mice (such as NCG or NSG strains).
- The Biology: This model provides a rapid wave of mature, functional human T cells (CD3+), including both CD4+ and CD8+ subsets. Because these cells are derived from an adult donor, they are already primed and highly responsive.
- The Catch (GvHD): Human T cells recognize the mouse major histocompatibility complex (MHC) molecules as foreign. This triggers a robust, systemic immune attack against the host tissues, known as Graft-versus-Host Disease. GvHD typically limits the experimental window to 3 to 4 weeks post-engraftment.
- Best Suited For: Short-term efficacy studies of T-cell engagers (TCEs), bispecific antibodies (BsAbs), and checkpoint inhibitors where immediate T-cell activation is the primary readout.
The hu-HSC Model
The hu-HSC model is created by irradiating or chemically conditioning immunodeficient neonates or young adult mice, followed by the transplantation of human CD34+ Hematopoietic Stem Cells (typically sourced from umbilical cord blood).
- The Biology: Unlike the hu-PBMC model, hu-HSC mice develop a complete, multi-lineage human immune system de novo. Over 10 to 12 weeks, these stem cells differentiate into human T cells, B cells, natural killer (NK) cells, and dendritic cells within the murine microenvironment.
- The Benefits: Because the human T cells mature within the mouse thymus, they undergo central tolerance selection, which drastically delays or prevents GvHD. This extends the study window to 6 months or longer.
- Best Suited For: Long-term combination therapies, safety and toxicity profiling, agents targeting myeloid cells (e.g., macrophage checkpoints like CD47), and tumor microenvironment (TME) architecture studies.
Target-Humanized Models (GEMMs)
Rather than transferring human cells, GEMMs utilize CRISPR/Cas9 or gene-targeting technologies to replace specific murine genetic sequences with their human counterparts (e.g., replacing murine PD-1 with human PD-1).
- The Biology: These mice retain a fully intact, fully functional murine immune system, but express humanized extracellular domains on specific immune checkpoints or receptors.
- The Benefits: Zero risk of GvHD, perfect physiological baseline immune responses, and maximum experimental reproducibility across cohorts.
- Best Suited For: High-throughput screening of monospecific monoclonal antibodies (mAbs) and evaluating standard checkpoint blockades where a fully native immune architecture is required.
The Decision Matrix
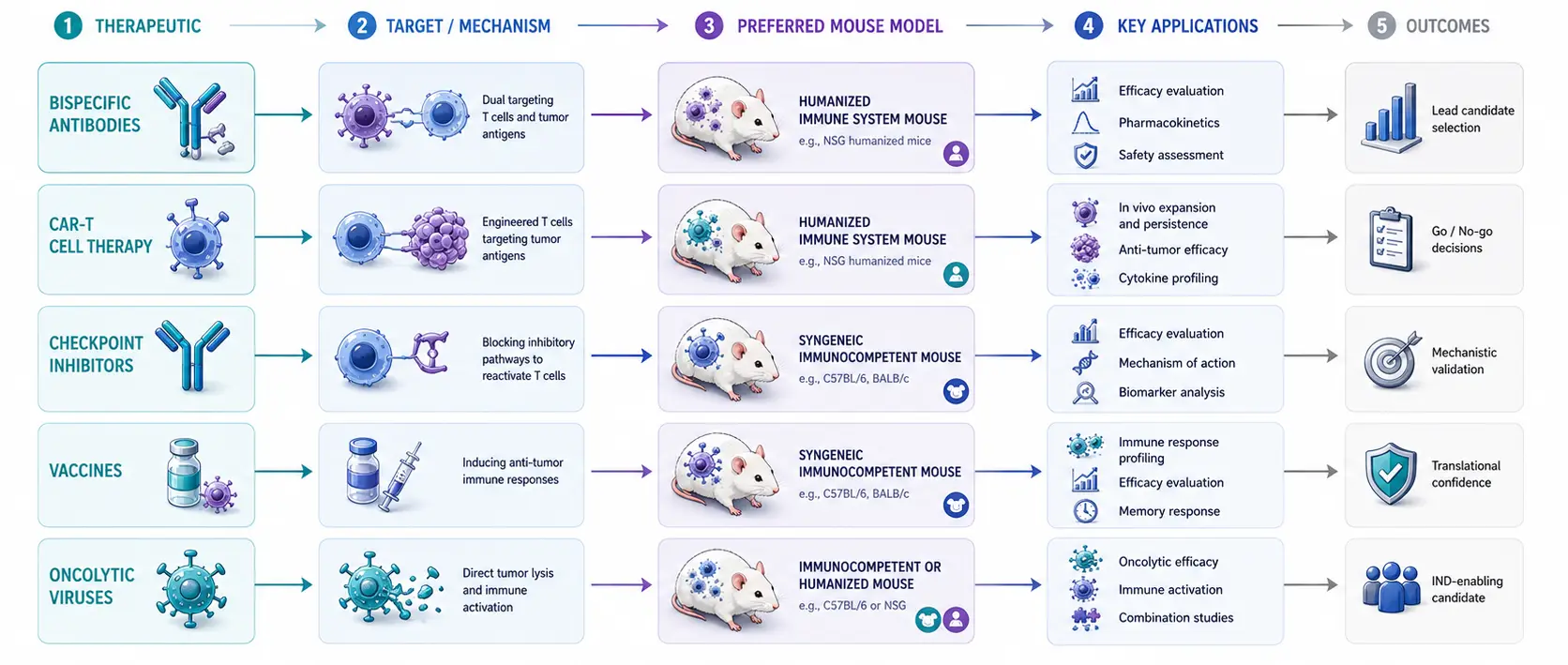
When matching your therapeutic asset to a model, a generic checklist will not suffice. Use the following decision matrix to cross-reference your specific modality with the optimal platform:
| Therapeutic Modality | Recommended Model | Primary Rationale | Critical Limitation |
|---|---|---|---|
| Bispecific T-Cell Engagers (TCEs) | hu-PBMC | Requires active, mature adult cytotoxic T cells for cross-linking. | GvHD onset creates a tight experimental window. |
| Myeloid / Macrophage Targets | Next-Gen hu-HSC | Transgenic human cytokines support human myeloid lineages. | High myeloid presence can sometimes cause anemia in the host. |
| CAR-T / Cell Therapy | Base Strain (NCG/NSG) | The therapeutic agent is the human immune cell; avoids cell competition. | Tumor models must be carefully chosen to avoid natural suppression. |
| Standard Checkpoint Inhibitors | GEMMs | Evaluates target blocking within a fully operational immune cycle. | Downstream signaling relies on murine components. |
The Unspoken Nuances: What Separates a Successful Study from a Flawed One?
When reviewing data or selecting a CRO partner, look beyond basic protocols. The following four operational variables determine whether your preclinical data will withstand regulatory scrutiny.
Donor-to-Donor Variability: The Biological Wildcard
Humanized mice carry the genetic diversity of human donors. The immune response profile can shift depending on the specific donor lot used for reconstitution.
The Solution: A rigorous protocol should always utilize multi-donor screening to ensure that drug efficacy data is reproducible across distinct donor cohorts.
Managing the Experimental Window
In hu-PBMC models, the precise synchronization of tumor inoculation, T-cell engraftment validation, and dosing initiation is critical. If tumor implantation occurs too late, GvHD-induced inflammation will mask the drug's true therapeutic effect.
Base Strain Selection
The background strain dictates the success of human cell engraftment. Strains carrying the Sirpα polymorphism or an IL-2 receptor common gamma chain (IL2rg) knockout-such as NCG or NSG-are superior hosts because they lack host NK, B, and T cells.
De-Risking Your Pipeline
Selecting a humanized mouse model is a customized strategic decision. Our portfolio of humanized platforms-spanning optimized hu-PBMC, deeply characterized hu-HSC cohorts, and an expansive catalog of target-humanized GEMMs-is backed by a team of immunologists dedicated to tailoring study designs to your drug's precise mechanism of action.
Ready to select the model for your next campaign? Contact our scientific team today for a complimentary technical consultation, or download our comprehensive Preclinical Model Selection Playbook.
Creative Bioarray Relevant Recommendations
| Products & Services | Description |
|---|---|
| Oncology Models | Creative Bioarray provides professional drug testing services using oncology disease models. Our disease models are suitable for testing new drugs or compounds that act on disease targets. |
| Humanized Mouse Models | Creative Bioarray enhances your preclinical immuno-oncology research endeavors by offering state-of-the-art humanized mouse model solutions that are tailored to target specific human immune responses. |
| Humanized PBMC Mouse Models | Creative Bioarray has successfully established highly stable humanized PBMC mouse models, tailored for our clients to evaluate the efficacy of immune therapies in tumor treatment. |
| Humanized CD34+ HSC Models | Creative Bioarray has successfully engineered sophisticated humanized mouse model featuring CD34+ hematopoietic stem cells (HSCs), meticulously designed for cutting-edge drug efficacy studies. |