Oncology Model Strategy: From Screening to Validation
In the high-stakes environment of oncology drug development, the most expensive mistake isn't a failed experiment-it's choosing a model that provides a "false positive." When preclinical data fails to translate into clinical results, the culprit is often a misalignment between the drug's mechanism and the biological platform used to test it.
This guide outlines a strategic framework for building a robust cancer model workflow, helping researchers navigate the transition from early-stage screening to IND-enabling validation.
The Strategic Foundation: Why "Workflow" Beats "Selection"
Many drug developers treat tumor model selection as a standalone task. However, a successful program relies on a continuous workflow. The goal is to create a "biological filter" that progressively increases complexity while maintaining data integrity.
A well-structured workflow addresses the three pillars of oncology testing:
- Sensitivity: Does the model possess the target?
- Context: Is the tumor microenvironment (TME) relevant to the drug's action?
- Translatability: Can the observed dose-response be modeled in humans?
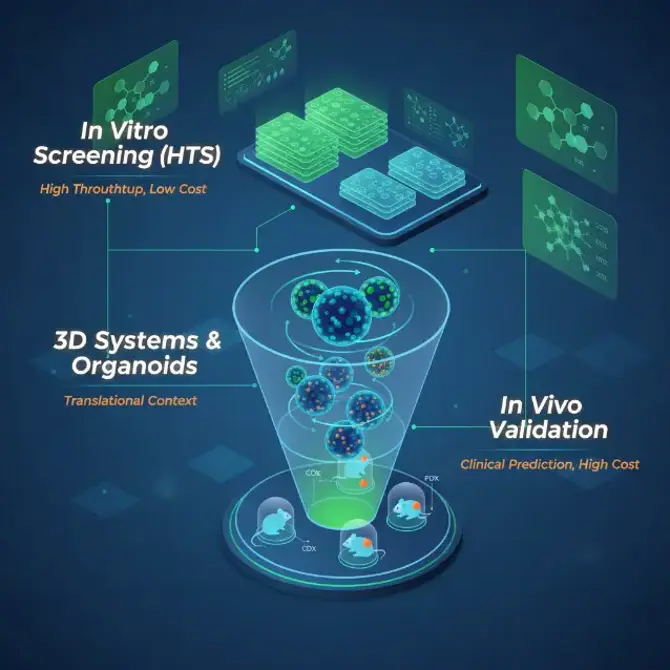
Phase I: In Vitro Optimization and 3D Systems
The screening phase is about defining the boundaries of your compound's activity.
The 2D vs. 3D Dilemma
Traditional 2D cell line screening is excellent for high-throughput baseline data. However, it fails to account for metabolic gradients and physical barriers.
Guidance: Use 2D for initial potency ranking across large panels. Transition to 3D systems (spheroids or organoids) as soon as you narrow down to lead candidates. 3D models provide a more accurate representation of drug penetration and resistance mechanisms, particularly for large molecules like ADCs.
Patient-Derived Organoids (PDOs)
PDOs are a game-changer for early validation. Because they maintain the genomic landscape of the original patient tumor, they allow for "clinical trials in a dish." Researchers should use PDOs to identify which genetic subtypes are most responsive, effectively creating a "molecular signature" for the drug before a single animal is dosed.
Phase II: Strategic In Vivo Model Selection
Choosing an animal model is not about finding the most "famous" mouse; it is about matching biology to mechanism.
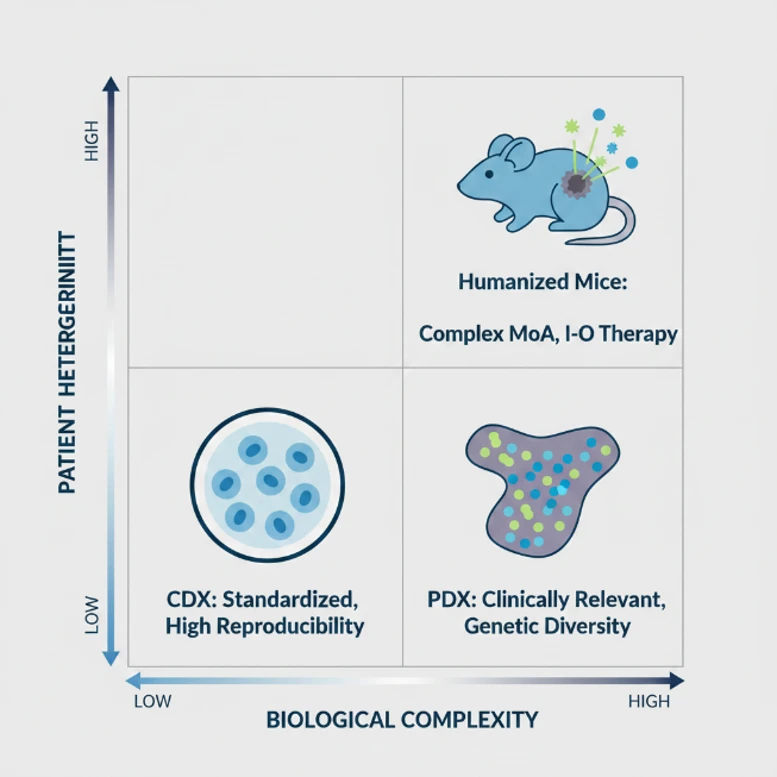
When to Use CDX (Cell Line-Derived Xenograft)
CDX models are the workhorses of oncology. They are highly standardized and offer low variability.
- Best Practice: Reserve CDX for early-stage PK/PD correlation and dose-finding studies. Their uniformity makes it easier to establish a statistically significant relationship between plasma concentration and tumor growth inhibition (TGI).
When to Transition to PDX (Patient-Derived Xenograft)
If your drug targets a specific mutation or relies on tumor heterogeneity, PDX is essential. PDX models capture the complex architecture of human tumors, including the stromal components that often drive resistance.
- Strategic Tip: Don't just pick any PDX. Use "Trial-Ready" PDX cohorts that have been pre-characterized via RNA-seq or Whole Exome Sequencing (WES) to ensure your target is expressed at clinically relevant levels.
The Immuno-Oncology (I-O) Decision Tree
For I-O agents, the host's immune system is the "second drug."
- Syngeneic Models: Best for testing broad-spectrum immune activators (like PD-1/L1 inhibitors) in an immunocompetent setting.
- Humanized Models (PBMC or HSC): Necessary for drugs that require human-specific targets (e.g., Bispecific T-cell Engagers or CAR-T). Researchers must be mindful of the "therapeutic window" here, as Graft-versus-Host Disease (GvHD) can complicate long-term efficacy reads.
Analytical Rigor: Translating Data into Decision Power
Generating a growth curve is only half the battle. To be truly instructive, the data must support a "Go/No-Go" decision for clinical entry.
PK/PD Integration
Efficacy data without pharmacokinetic context is dangerous. A compound might show high TGI simply because the dose is near the Maximum Tolerated Dose (MTD), which may not be achievable in humans.
- Instruction: Always measure "Target Engagement." If your drug inhibits a kinase, demonstrate that the phosphorylation of that kinase is actually reduced within the tumor tissue, not just in peripheral blood.
Biomarker Identification
Preclinical validation should yield a "Predictive Biomarker." By performing post-study analysis (FACS, IHC, or Omics) on responding vs. non-responding models, you can identify the specific biological traits that correlate with success. This allows clinical teams to design "Enrichment Trials," selecting patients most likely to benefit and significantly reducing the risk of a Phase II failure.
Methodological Pitfalls: What to Avoid
Even with the right model, execution errors can derail a program.
- Ignoring the "Cold" Tumor: Many syngeneic models are "hot" (highly inflamed), making it too easy for a drug to show efficacy. Ensure your strategy includes "cold" (immune-excluded) models to challenge your drug's ability to recruit immune cells.
- Over-reliance on TGI: Tumor Growth Inhibition is a snapshot. Look for "Recurrence Rates" after dosing has stopped. A drug that causes regression followed by immediate relapse may require a different combination strategy.
- Standard of Care (SoC) Comparison: Never test your drug in isolation. To demonstrate value to regulators and investors, you must show how it performs relative to, or in combination with, current Standard of Care treatments.
Summary: The Preclinical-to-Clinical Bridge
A successful oncology drug testing program is defined by its ability to predict human outcomes. By shifting from a "box-ticking" exercise to a mechanism-driven Oncology Model Strategy, researchers can ensure that their preclinical data is not just an endpoint, but a reliable compass for the clinical journey ahead.
The focus must always remain on biological relevance. Whether it's choosing between a CDX or PDX, or deciding when to move into humanized systems, the guiding question should always be: Does this model represent the patient we intend to treat?
Key Takeaways for Researchers:
- Identify the MoA early: Let the drug's mechanism dictate the model.
- Progressive Complexity: Use 2D/3D screening to inform animal model selection.
- Focus on PD: Prove target engagement to justify the dose.
- Think Clinically: Use preclinical models to find your future patient biomarkers.
Creative Bioarray Relevant Recommendations
| Products & Services | Description |
|---|---|
| Oncology Models | Creative Bioarray provides professional drug testing services using oncology disease models. Our disease models are suitable for testing new drugs or compounds that act on disease targets. |
| Tumor Cell Models | Creative Bioarray offers a variety of in vitro platforms for your oncology research program. |