
Renal Proximal Convoluted Tubule Epithelial Cells
Cat.No.: CSC-7637W
Species: Human
Source: Kidney
Cell Type: Epithelial Cell
- Specification
- Background
- Scientific Data
- Q & A
- Customer Review
These primary RPCTs are collected from unfractionated kidney cell preparations from normal, non-diseased human kidney tissues. The cells can be cultured and expanded in Bioarray's unique renal epithelial cell culture media formulations delivering a robust renal cell culture for use in experiments and screening assays.
Bioarray provides RPCTs cryopreserved at 500,000 cells/vial along with 50ml of RPCT plating media for each vial to establish initial culture. Purity of each lot is verified using morphology and CD13 flow cytometry – Bioarray RPCTs are qualified at >80% CD13+ upon QC release.
Each lot of primary renal cells are tested and verified negative for HIV-1, HIV-2, HTLV I & II, Hep B & C, Syphillis and CMV.
Custom donor specifications are available upon request and a number of different plate and flask formats can be customized to meet your particular research project needs.
RPTECs, or renal proximal convoluted tubule epithelial cells, are primary cells originating from the proximal section of the nephron, the kidney's main site for reabsorption and metabolic conversion. They create a polarized monolayer with large brush boundaries (microvilli) to maximize surface area for transport. RPTECs maintain important functional indicators such as alkaline phosphatase and megalin in culture, but require specialized serum-reduced medium to preserve their differentiated phenotype and tight junction integrity when cultured at typical 37°C, 5% CO2 conditions.
Their main value is in toxicology and drug development, as the gold standard for prediction of drug-induced kidney injury (DIKI), and nephrotoxicity screening. They are required to research renal drug transport kinetics, including uptake by OATs and OCTs, and efflux by P-gp, which defines the systemic drug clearance. RPTECs are also utilized to model diabetic nephropathy by exposing to high glucose to develop fibrosis and albuminuria. RPTECs may also be employed to study processes of acute kidney injury (AKI) involving oxidative stress and mitochondrial dysfunction. They are additionally frequently utilized in transporter-mediated drug-drug interaction (DDI) studies to assure pharmaceutical safety.
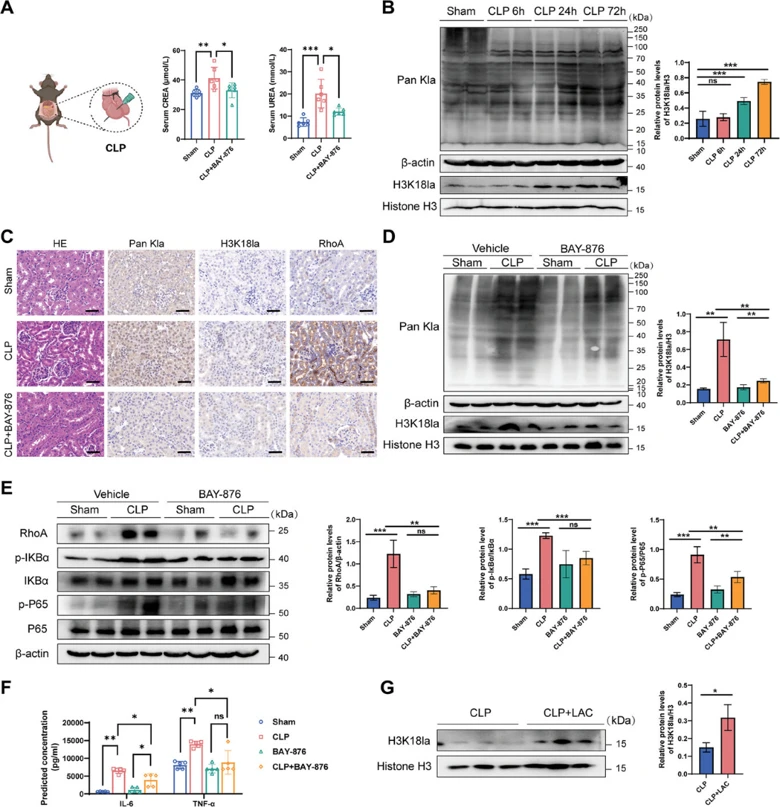
Histone Lactylation Drives Inflammatory Injury in Sepsis-Associated AKI
Histone lactylation is a metabolite-driven modification whose role in sepsis-associated acute kidney injury (SA-AKI) is unknown. Qiao et al. elevated histone H3K18 lactylation (H3K18la) in SA-AKI.
Clinical data link high serum lactate to sepsis severity. In a murine CLP model, serum lactate, creatinine, and urea nitrogen rose significantly (Fig. 1A). Renal histone lactylation peaked at 24 h post-CLP and remained elevated through 72 h, mirroring the kinetic profile of H3K18la (Fig. 1B). Immunohistochemistry localized this modification primarily to the nuclei of proximal convoluted tubule epithelial cells (Fig. 1C). To assess functional relevance, mice were pretreated with BAY-876 (a glycolysis inhibitor) 24 h prior to CLP. BAY-876 suppressed global renal lactylation and H3K18la, downregulated RhoA and the NF-κB pathway (reduced IKBα and NF-κB phosphorylation), and lowered IL-6 and TNF-α levels (Fig. 1D-F). Histology confirmed reduced H3K18la and inflammatory infiltration (Fig. 1C). Conversely, elevating systemic lactate via peritoneal injection increased renal H3K18la levels (Fig. 1G).
Collectively, these data demonstrate that increased H3K18la activates the NF-κB pathway and exacerbates kidney injury, while its reduction mitigates inflammation and improves renal outcomes in SA-AKI.
Ask a Question
Write your own review

Description: Renal glomerular endothelial cells (GEC) are a specialized microvascular cell type involved in the regulation of glomerular ultrafiltration. They form the inner part of the filtration barrier and are ...

Description: Human Kidney Endothelial Cells from Creative Bioarray are isolated from human kidney tissue. Human Kidney Endothelial Cells are grown in T25 tissue culture flasks pre-coated with gelatin-based ...
Description: Human Proximal Tubular Epithelial Cells from Creative Bioarray are isolated from normal human proximal tubular tissue. Human Proximal Tubular Epithelial Cells are grown in T25 tissue culture flasks ...
Description: Primary Human Glomerular Microvascular Endothelial Cells were initiated by decapsulated glomeruli isolated from normal human kidney cortical tissue.These cells were originated using Complete ...
Description: Human Kidney Carcinoma Epithelial Cells from Creative Bioarray are isolated from human kidney tumor tissue. Human Kidney Carcinoma Epithelial Cells are grown in T25 tissue culture flasks pre-coated ...

Description: VE-Cad-GFP Expressing Human Glomerular Microvascular Endothelial Cells (VE-Cad-GFP HGMvECs) provided by Creative Bioarray are puromycin-selected from Human Glomerular Microvascular Endothelial Cells ...