
Renal Mixed Epithelial Cells, Primary, 500,000 cells per vial
Cat.No.: CSC-C4068X
Species: Human
Source: Kidney
Cell Type: Epithelial Cell
- Specification
- Background
- Scientific Data
- Q & A
- Customer Review
Cell Features:
Mixed Renal Epithelial, Renal Cortical Epithelial, and Renal Medullary Epithelial are cryopreserved as primary cells isolated from human kidney tissue and expanded in culture vessels once before cryopreservation.
Renal Proximal Tubule Epithelial are cryopreserved as secondary cells isolated from human kidney tissue and expanded in culture vessels twice before cryopreservation.
All Renal Epithelial Cell types can be grown in a 0.5% serum medium without phenol red or antimicrobials when cultured in LIRen Medium.
All Renal Epithelial Cell types are extensively tested for quality and optimal performance.
Creative Bioarray guarantees performance and quality.
Primary Human Renal Mixed Epithelial Cells, as their name suggests, are an epithelial cell population derived directly from normal kidney tissue. These cells are "primary" because they are not immortalized cell lines. As a result, they maintain the phenotype of the tissue from which they are derived and tend to demonstrate morphology and functionality more relevant to the in vivo state.
Mixed epithelial cells obtained from the kidney are cobblestone in appearance and express epithelial cell markers such as Cytokeratin and E-cadherin. Since they are comprised of many different cell types originating from the nephron (proximal tubules, distal tubules, collecting ducts, etc.), they can be used to study cellular interactions between multiple cell types. Typical applications of these cells include:
- Detection of Nephrotoxicity: Determine how cells respond to potential pharmaceutical drugs and environmental chemicals.
- Renal Transport/Metabolism: Examination of transporters, electrolyte homeostasis, and metabolism.
- Disease Modeling: Mechanisms of acute kidney injury (AKI), chronic kidney disease (CKD), fibrosis, etc.
- Tissue Engineering: Cell therapy and tissue engineering studies.
These cells have limited lifespans due to their primary nature and require rich growth media containing hormones and growth factors to sustain their differentiated phenotype in culture. They act as an intermediary between standard cell culture and animal models.
Combination Treatment with PAC and ATRA Synergistically Inhibits the Proliferation of ADPKD Cells but Not HRECs
Autosomal dominant polycystic kidney disease (ADPKD) is characterized by uncontrolled epithelial cell growth, cyst formation, and kidney malfunction. Nguyen et al. investigated the antiproliferative effects of combining paclitaxel (PAC) and all-trans retinoic acid (ATRA) on ADPKD epithelial cells.
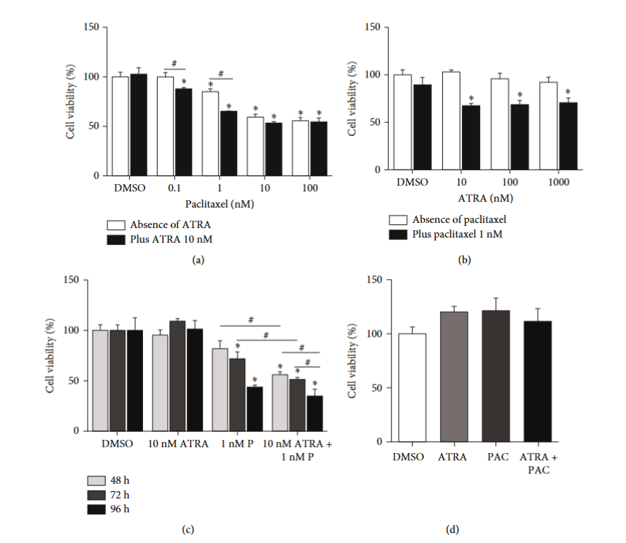
To find the optimal concentrations for combination treatment, cells were treated with various concentrations of PAC and ATRA. Treatment with 10 nM PAC alone reduced cell viability by 40% (Fig. 1a), while ATRA alone (10-1000 nM) had no significant effect (Fig. 1b). Fixing ATRA at 10 nM, they tested different PAC concentrations and found that 1 nM PAC combined with ATRA showed the most potent inhibitory effect (20% reduction in cell viability) compared to PAC alone. Other PAC concentrations were less effective (Fig. 1a). Fixing PAC at 1 nM, we confirmed the maximum inhibitory effect with at least 10 nM ATRA (Fig, 1b). These optimal concentrations (1 nM PAC and 10 nM ATRA) were verified with different incubation periods (Fig. 1c). Subsequent experiments used this combination (PAC+ATRA). PAC+ATRA did not affect primary normal human renal mixed epithelial cells (HRECs) viability (Fig. 1d), ensuring selective action on ADPKD cells. A wound healing assay showed that PAC+ATRA significantly slowed wound gap closure compared to DMSO controls (Fig. 1e and 1f), indicating suppression of ADPKD cell proliferation and migration.
Ask a Question
Write your own review

Description: Renal glomerular endothelial cells (GEC) are a specialized microvascular cell type involved in the regulation of glomerular ultrafiltration. They form the inner part of the filtration barrier and are ...

Description: Human Kidney Endothelial Cells from Creative Bioarray are isolated from human kidney tissue. Human Kidney Endothelial Cells are grown in T25 tissue culture flasks pre-coated with gelatin-based ...
Description: Human Proximal Tubular Epithelial Cells from Creative Bioarray are isolated from normal human proximal tubular tissue. Human Proximal Tubular Epithelial Cells are grown in T25 tissue culture flasks ...
Description: Primary Human Glomerular Microvascular Endothelial Cells were initiated by decapsulated glomeruli isolated from normal human kidney cortical tissue.These cells were originated using Complete ...
Description: Human Kidney Carcinoma Epithelial Cells from Creative Bioarray are isolated from human kidney tumor tissue. Human Kidney Carcinoma Epithelial Cells are grown in T25 tissue culture flasks pre-coated ...

Description: VE-Cad-GFP Expressing Human Glomerular Microvascular Endothelial Cells (VE-Cad-GFP HGMvECs) provided by Creative Bioarray are puromycin-selected from Human Glomerular Microvascular Endothelial Cells ...