Dental Follicle Stem Cells
- Specification
- Background
- Scientific Data
- Q & A
- Customer Review
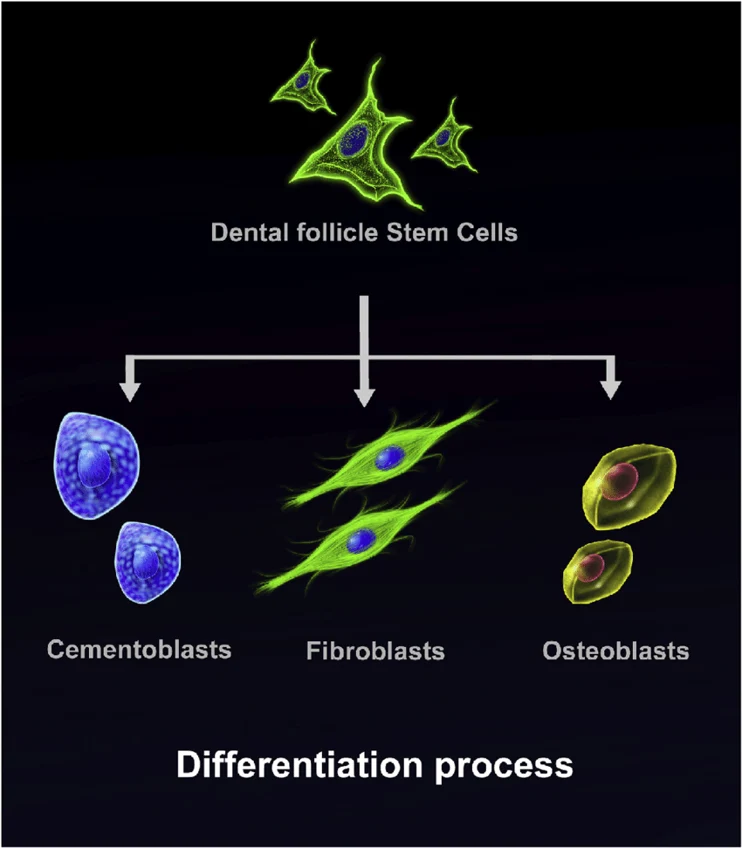
Dental Follicle Stem Cells (DFSCs) are multipotent mesenchymal stem cells extracted from the dental follicle which envelops the tooth germ. DFSCs are neural crest-derived population of stem cells with robust proliferative ability and high self-renewal potential.
DFSCs are fibroblast-like in morphology, showing a spindle-shape when plated, and can be cultured as adherent monolayers. These cells are positive for mesenchymal markers including CD73, CD90, and CD105 and are negative for hematopoietic lineage markers like CD34 and CD45. DFSCs are able to differentiate into osteogenic, adipogenic, chondrogenic, and cementoblastic lineages with proper induction. Due to their ability to generate tooth development and periodontal tissues like cementum, periodontal ligament, and alveolar bone, DFSCs are utilized to model craniofacial development, stem cell differentiation, and tooth related tissue engineering. Dental follicle stem cells have also shown immunomodulatory capabilities along with biocompatibility making them useful for cell-based therapies.
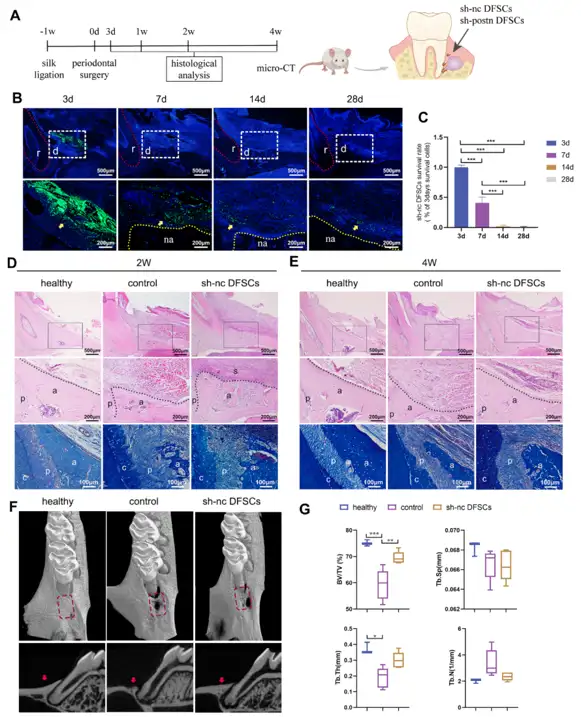
DFSCs Significantly Promoted Periodontal Regeneration while the Cell Survival Rate Was Low after Transplantation
Dental follicle stem cells (DFSCs) promote periodontal repair in inflamed tissues, yet their poor survival suggests paracrine factors are key. Wei's team investigated whether periostin-highly expressed by DFSCs under inflammation-mediates this regenerative effect and explored its therapeutic potential.
An experimental periodontitis model was established in SD rats by ligation and bacterial coating, followed by creation of periodontal intrabony defects and transplantation of GFP-labeled DFSCs (sh-nc DFSCs) (Fig. 1A). GFP tracking revealed abundant cells at 3 days, ~40% retention at 7 days, and <5% survival at 2-4 weeks (Fig. 1B, C). Notably, GFP⁺ DFSCs did not differentiate into osteocytes, periodontal ligament cells, or cementoblasts, but remained localized around regenerating tissues (Fig. 1B). Despite poor long-term survival, DFSCs significantly enhanced periodontal regeneration. At 2 weeks, the sh-nc DFSCs group showed superior bone formation with orderly periodontal ligament arrangement compared to disorganized controls (Fig. 1D). By 4 weeks, DFSC-treated defects exhibited dense, plump alveolar bone comparable to healthy tissue, whereas controls displayed minimal bone filling with collapsed soft tissue (Fig. 1E). Micro-CT confirmed significantly higher BV/TV in the sh-nc DFSCs group versus controls, with no difference from healthy rats (Fig. 1F, G), indicating DFSCs promote periodontal regeneration despite limited engraftment.
Ask a Question
Write your own review
- Adipose Tissue-Derived Stem Cells
- Human Neurons
- Mouse Probe
- Whole Chromosome Painting Probes
- Hepatic Cells
- Renal Cells
- In Vitro ADME Kits
- Tissue Microarray
- Tissue Blocks
- Tissue Sections
- FFPE Cell Pellet
- Probe
- Centromere Probes
- Telomere Probes
- Satellite Enumeration Probes
- Subtelomere Specific Probes
- Bacterial Probes
- ISH/FISH Probes
- Exosome Isolation Kit
- Human Adult Stem Cells
- Mouse Stem Cells
- iPSCs
- Mouse Embryonic Stem Cells
- iPSC Differentiation Kits
- Mesenchymal Stem Cells
- Immortalized Human Cells
- Immortalized Murine Cells
- Cell Immortalization Kit
- Adipose Cells
- Cardiac Cells
- Dermal Cells
- Epidermal Cells
- Peripheral Blood Mononuclear Cells
- Umbilical Cord Cells
- Monkey Primary Cells
- Mouse Primary Cells
- Breast Tumor Cells
- Colorectal Tumor Cells
- Esophageal Tumor Cells
- Lung Tumor Cells
- Leukemia/Lymphoma/Myeloma Cells
- Ovarian Tumor Cells
- Pancreatic Tumor Cells
- Mouse Tumor Cells