
Human Cardiomyocytes
Cat.No.: CSC-C2847
Species: Human
Source: Heart
Cell Type: Cardiomyocyte
- Specification
- Background
- Scientific Data
- Q & A
- Customer Review
Cardiomyocytes may be used in various in vitro or in vivo studies; transplantation into normal or diseased systems; cardiac toxicology studies; or cardiovascular developmental studies.
Cardiovascular disease remains the leading cause of mortality worldwide, claiming more than 17 million lives each year and contribute to a huge economic burden. Therefore, both the study of disease mechanisms and cardiovascular drug discovery are fundamental to alleviating this increasing burden.
Despite significant advances in cardiac modeling over the past few decades, adequate cardiac models are still lacking for cardiovascular research and drug discovery. Currently, rodent models remain ideal for in vivo studies, while human pluripotent stem cell (hPSC)-derived cardiomyocytes (hPSC-CMs) have become one of the most popular in vitro models in recent years. hPSC-CMs are now widely used in both basic research and preclinical safety pharmacology and have greatly improved our understanding of the physiology, pathology, and pharmacology of the human heart. However, hPSC-derived cells exhibit immature phenotypes in many aspects, including cellular structure, gene expression, metabolism, and electrophysiology, which are the current directions of efforts. By contrast, human primary cardiomyocytes (hPCMs) isolated directly from human heart tissue, possess all the elements required for a cellular model (e.g., native structure and function, patient-specific genetic and epigenetic information, etc.), and thus is theoretically an ideal cell model.
Table 1. The differences between hPSC-CMs and hPCMs.
| hPSC-CMs | hPCMs | |
| Cell population | Mixed/Unreliable | Pure/Reliable |
| Morphology | Irregular | Rod-shaped |
| Cell maturity | Immature | Adult |
| Contraction | Spontaneous | Electrical pacing |
| Contraction force | Reduced | Significant |
| Sarcomeric structure | Disorganized | Organized |
| T-tubule structure | Deficient | Abundant |
| Ryanodine receptor distribution | Heterogenous | Homogenous |
| Ion channel expression | Under- or over-expressed | Physiological |
| Ca2+ handling | Functional yet immature | Functional fully mature |
| Force-frequency relationship | Negative | Positive |
| Post-rest potentiation | Absent or weak | Present |
Cardiomyocyte Isolation from Frozen Human Tissue
An overview of the isolation method is shown in Fig. 1A. Tissue was thawed and cut into 1 mm3 pieces while submerged in ice-cold wash solution (115 mM potassium gluconate, 2.5 mM potassium chloride (KCl), 5 mM potassium phosphate monobasic (KH2PO4), 2 mM magnesium sulfate (MgSO4), 2 mM calcium chloride (CaCl2), 30 mM sucrose, 10 mM 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES), pH 7.4). Tissue pieces were collected with a 70 μm cell strainer and washed three times with ice-cold wash solution. Tissue pieces were placed in digestion solution (300 Units/mL collagenase type 4, 5 Units/mL DNase I, and 1 mg/mL trypsin inhibitor in wash solution) in a 50 mL spinner flask at 37 °C. A total of three digestions were performed, each yielding a fraction of crude cardiomyocytes that was filtered through a 200 μm cell strainer. Crude cardiomyocytes from three digestions were combined, collected by centrifugation at 80 ×g for 5 min at 4 °C, and washed three times in ice-cold wash solution. Crude cardiomyocytes were further purified by removing immune cells and endothelial cells by negative selection. Isolated cardiomyocytes were assessed for percent troponin I (TNNI3) positivity by flow cytometry. Visual assessment of cardiomyocytes using immunofluorescent labeled cardiac actin was performed on a confocal laser scanning microscope.
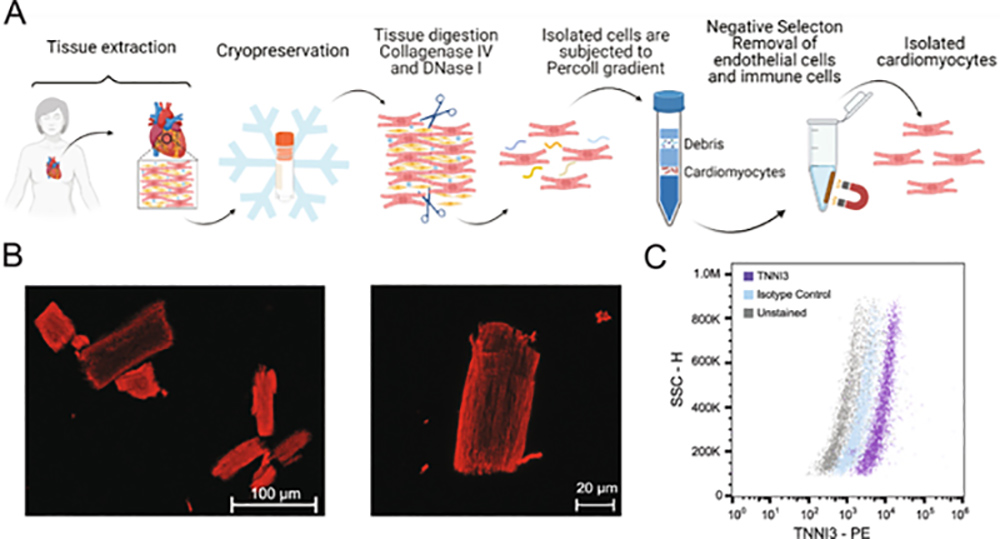 Fig. 1. Cardiomyocyte isolation and purity assessment. A) Schematic overview of cardiomyocyte isolation workflow using cryopreserved human adult cardiac tissue. B) Representative confocal immunofluorescence images of isolated cardiomyocytes stained for cardiac actin (red). C) Flow cytometry assessment of isolated cells for TNNI3 positivity (Wojtkiewicz, M. et al., 2022).
Fig. 1. Cardiomyocyte isolation and purity assessment. A) Schematic overview of cardiomyocyte isolation workflow using cryopreserved human adult cardiac tissue. B) Representative confocal immunofluorescence images of isolated cardiomyocytes stained for cardiac actin (red). C) Flow cytometry assessment of isolated cells for TNNI3 positivity (Wojtkiewicz, M. et al., 2022).
Cardiomyocyte Contractility Measurement
With the ultimate goal of assessing both electrical (AP) as well as mechanical (contractility) drug-induced effects, we decided to focus our analysis on four parameters: TR90 (time to 90% relaxation; ms), incidence of AC (after-contraction), incidence of CE (contractility escape) and sarcomere shortening. TR90 is correlated to the duration of the cardiac AP and delays in AP repolarization are expected to be associated with extension of the TR90. Early-afterdepolarization (EAD) is an AP abnormality that results in a transient slope change of the AP during the repolarization phase. EAD is potentially of great relevance in the context of pro-arrhythmia risk assessment since this is believed to be the underlying cause of re-entrant arrhythmia. The mechanical equivalent of EAD electrical abnormality is an after-contraction, a transient change of slope in the contractility transient, typically in the later portion of the relaxation phase. Drugs that interfere with cardiac depolarization or in other ways suppress the generation of a cardiac AP, result in complete inhibition of the contractility transient, an event we refer to as CE. Therefore, changes in three parameters measured from contractility transients, TR90, AC and CE can provide useful information with regards to the drug-induced alterations of the electrical behavior of cardiac cells. In addition, changes in fractional sarcomere shortening provide direct measurement of inotropic effects in cardiomyocytes.
We recorded vehicle time-control data in four cardiomyocytes (one heart) using multiple additions of vehicle solution spaced by 4 min each, to mimic the experimental conditions that we were set to use with the test drugs. Cardiomyocytes exhibited stable behavior for the duration of the recordings, up to 20 min (Fig. 2). No AC or CE were observed and only a small, non-significant increase in TR90 was observed (Fig. 2A). Similarly, the measurements of sarcomere shortening in myocytes demonstrated good stability (Fig. 2B).
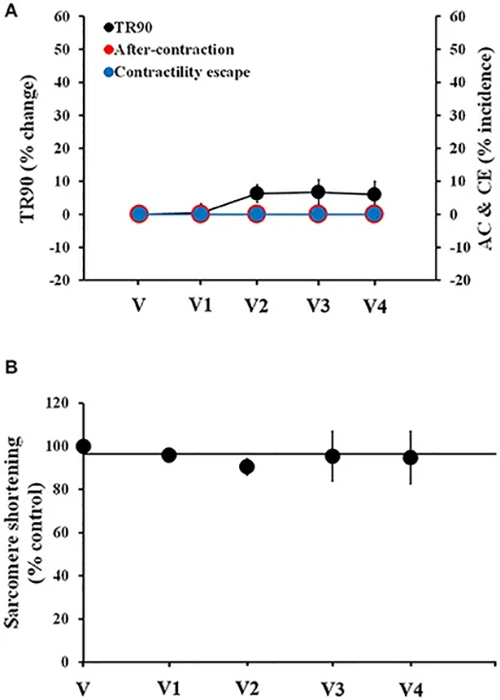 Fig. 2. Stability of contractility recordings over time in human cardiomyocytes. (A) Change in TR90 and % incidence of AC and CE induced by sequential additions of vehicle (V) in human cardiomyocytes at 1 Hz pacing frequency. (B) Vehicle effect curve for sarcomere shortening (Nguyen, Nathalie, et al., 2017).
Fig. 2. Stability of contractility recordings over time in human cardiomyocytes. (A) Change in TR90 and % incidence of AC and CE induced by sequential additions of vehicle (V) in human cardiomyocytes at 1 Hz pacing frequency. (B) Vehicle effect curve for sarcomere shortening (Nguyen, Nathalie, et al., 2017).
Functional Characterization of Freshly Isolated hPCMs
First, we used patch clamping to characterize major membrane currents and their responses to specific inhibitors. Sodium currents were elicited by a series of depolarizing test potentials between −120 to +100 mV with 30 mV steps at a holding potential of −120 mV. The peak density of sodium current was at −20 mV, and the mean maximal peak INa normalized to cell capacitance was −39.27 ± 14.50 pA/pF (n = 10) (Fig. 3a). We also characterized the voltage-dependent steady-state activation and inactivation curves of sodium currents. The voltage at half activation (V1/2) was −35.07 ± 0.87 mV (n = 10), with a mean slope factor (k) of 3.43 ± 0.76, whereas the V1/2 for inactivation −72.13 ± 0.54 mV (n = 10), and the slope factor was 4.30 ± 0.47 (Fig. 3b, c). Time-dependent recovery of sodium currents from inactivation was assessed using a paired-pulse protocol. The mean recovery time constant of sodium currents was 3.83 ± 0.35 ms (n = 10) (Fig. 3d). Likewise, L-type Ca2+ currents (ICa,L) currents were elicited at potentials between −60 to +90 mV, with 30 mV steps at a holding potential of −80 mV. The I–V relationship showed that the peak density of calcium currents occurred at 30 mV, and the mean maximal peak ICa,L normalized to cell capacitance was −3.66 ± 0.98 pA/pF (n = 4) (Fig. 3e). We further characterized the current–voltage (I–V) relationships of two major potassium currents in freshly isolated hPCMs. For the 4-aminopyridine (4-AP)-sensitive, non-Ca2+-dependent transient outward potassium current (Ito), its current density averaged −0.13 ± 0.24 pA/pF at −40 mV, 2.17 ± 1.06 pA/pF at 0 mV, and 12.96 ± 4.32 pA/pF at +40 mV (Fig. 3f). The ultrarapid outward current Ikur is the other major repolarizing current in the human atrium. Ikur density averaged 0.24 ± 0.16 pA/pF at −40 mV, 2.00 ± 1.23 pA/pF at 0 mV, and 5.28 ± 3.39 pA/pF at +40 mV (Fig. 3g). Together, these data demonstrate proper ionic currents of isolated hPCMs.
To further validate the functionality of cardiomyocytes, we tested whether these currents responded correctly to specific channel inhibitors. To this end, we used tetrodotoxin (TTX), nifedipine, and 4-aminopyridine (4-AP) to respectively inhibit Na+ (INa), Ca2+ (ICa), and K+ (Ito) currents (Fig. 3h-j). The half-maximal inhibitory concentration (IC50) values for TTX, nifedipine, and 4-AP were 16.24 μM, 55.39 nM, and 0.2563 mM, respectively, which were similar to reports in the literature (Fig. 3k-m). Taken together, isolated hPCMs exhibited normal electrophysiology, indicating their potential use as models to evaluate drugs that affect the electrical properties of cardiomyocytes.
We next used isoproterenol and norepinephrine to examine whether cells responded to neurohormonal stimulation. Both stimuli caused time- and dose-dependent increases in the phosphorylation of phospholamban, an important regulator of calcium handling in cardiomyocytes (Fig. 3n), demonstrating that cells retained functional adrenergic signaling following isolation.
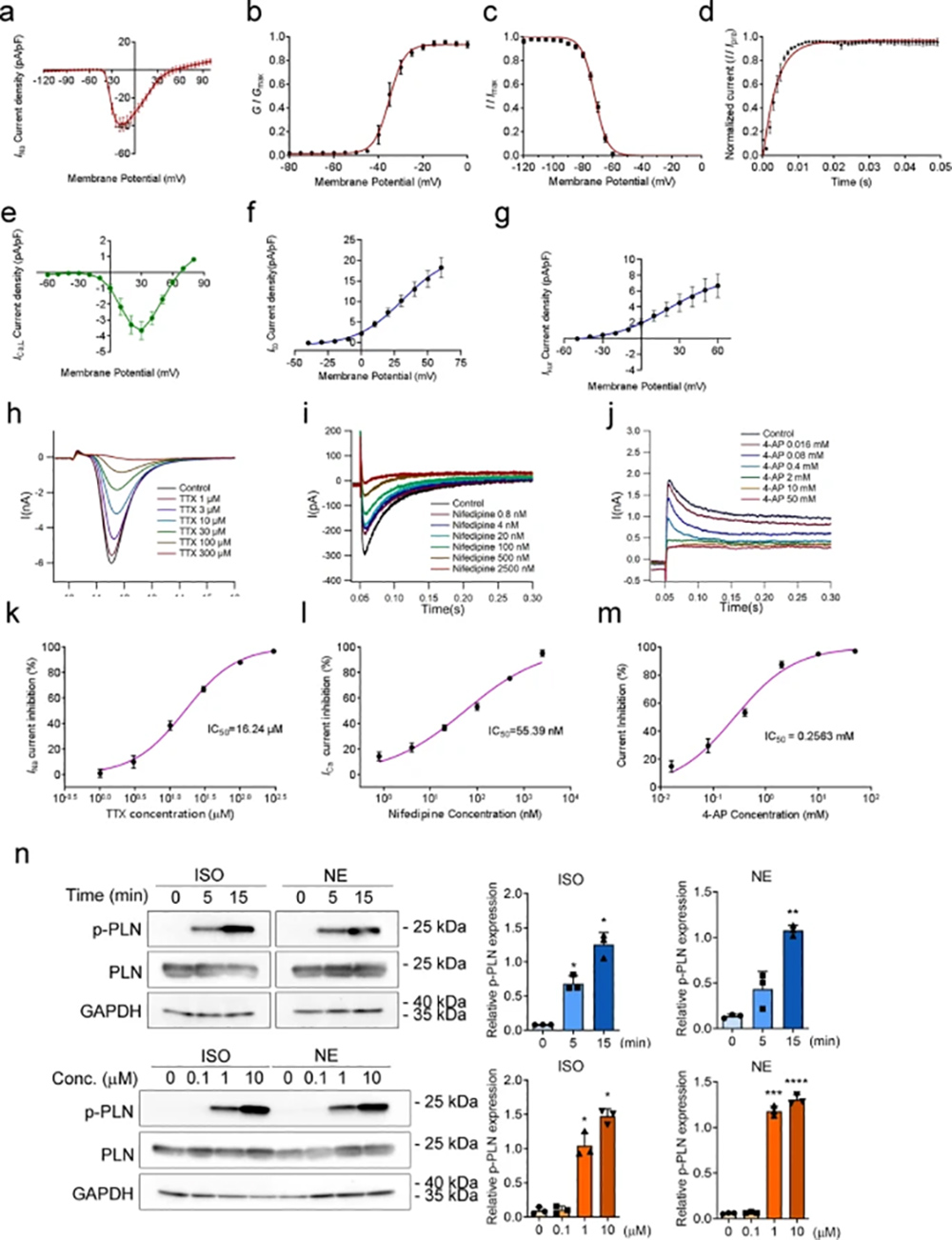 Fig. 3. Functional integrity of freshly isolated hPCMs (Zhou, Bingying, et al., 2022).
Fig. 3. Functional integrity of freshly isolated hPCMs (Zhou, Bingying, et al., 2022).
Actually, we have two types of Human Cardiomyocytes: tissue-derived and iPSC-derived. The tissue-derived cardiomyocytes are isolated from normal human ventricle tissue of the adult heart. They are guaranteed for 15 population doublings with a doubling time of 34.5h. The cells are cryopreserved at P2, so they'll be P3 when you start culture them. These cardiomyocytes don't beat in the culture. The iPSC-derived cardiomyocytes can be maintained in culture for an extended duration. We have cultured the cells for 1 year and the cells still maintain the beating phenotype and gene expression patterns.
We can provide two kinds of human cardiomyocytes, tissue-derived and iPSC-derived. However, we haven't tested them for beta 1 adrenergic receptor expression.
The tissue-derived cardiomyocytes are isolated from normal human ventricle tissue of the adult heart.
Since the cells are isolated from donated tissues and the amount of cells from a single donor is limited, we run out of the cells from the same donor every now and then. Therefore, we cannot guarantee that the cells you order each time will from the same donor. We might be able to reserve 1 or 2 vials for you when you place your first order, but the reservation can stay valid for a month or two.If it's necessary for you to use cardiomyocytes continuously from the same origin, I would like to recommend to you our cardiomyocytes derived from iPS cells. These cells are quite stable and they are able to maintain their beating morphology if cultured with our optimized media.
Human primary cardiomyocytes are frequently used in research and drug development to study the underlying mechanisms of heart disease, test the efficacy and safety of new drugs, and evaluate potential treatments for various cardiac conditions. These cells can be used to model heart diseases such as cardiomyopathy, arrhythmias, and heart failure, and to screen for drug-induced cardiotoxicity.
Human primary cardiomyocytes can be isolated from heart tissue obtained from organ donors, patients undergoing heart surgery, or induced pluripotent stem cells (iPSCs) derived from patient samples. These cells are cultured in the laboratory and can be used for a wide range of experiments to better understand the biology of the heart and develop new therapeutic strategies for heart disease.
One of the major challenges of using human primary cardiomyocytes is their limited availability and variability between donors. These cells also have a relatively short lifespan in culture and can be difficult to maintain their physiological properties over time. Additionally, the cost of obtaining and culturing human primary cardiomyocytes can be high, which can limit the scope and scale of experiments that can be conducted.
Ask a Question
Average Rating: 5.0 | 1 Scientist has reviewed this product
Excellent
The cells were highly viable and showed excellent morphology under the microscope. I would definitely recommend these human primary cardiomyocytes to other researchers.
2 Aug 2022
Ease of use
After sales services
Value for money
Write your own review

Description: HPcF from Creative Bioarray are isolated from the human heart. HPcF are cryopreserved at secondary culture (passage one) and are delivered frozen. Each vial contains >5 x 10^5 cells in 1 ml volume. ...

Description: Human hypertension cardiac microvascular endothelial cells from Creative Bioarray are isolated from the heart of human donor that has been diagnosed with hypertension. Human Hypertension Cardiac ...
Description: HAAF from Creative Bioarray Research Laboratories are isolated from human aortic artery. HAAF are cryopreserved at first passage of primary culture and delivered frozen. Each vial contains >5 x 10^5 ...
Description: Creative Bioarray has developed Human iPSC-Derived Cardiomyocytes, in addition to our human cardiomyocytes isolated from fresh heart tissue. Human iPSC-Derived Cardiomyocytes overcome the limitations ...
Description: HCF from Creative Bioarray Research Laboratories are isolated from the human heart. HCF-a are cryopreserved at secondary culture and delivered frozen. Each vial contains >5 x 10^5 cells in 1 ml ...
Description: Cardiac progenitor cells are derived from the heart (of a single donor) that has been dissociated into single cells and cultured using differential adhesion. These cells are characterized by ...